
The term “Ocular Tuberculosis” is defined as an extra-pulmonary form of the disease that includes any infection in or around the eye caused due to Mycobacterium tuberculosis. It may be either active infection or an immunologic reaction, related to delayed hypersensitivity (an aseptic reaction to tubercular antigen).Ocular Tuberculosis is categorised into two types, in case of primary ocular TB: the eye is the initial port of entry into the body, and for secondary one, the infection spreads via the bloodstream from a distant site or a direct invasion from adjacent areas like the sinus or the cranial cavity.In Ocular Tuberculosis, every tissue of the eye can get affected. The patient suffering from Ocular TB , if untreated, usually runs a chronic course with exacerbations and remissions.
Following are a few cases that have been treated at Uvea Clinic, Neoretina:
Case 1. A 55 year old lady presented with sudden loss of vision in her left eye since 10 days. On examination her left eye showed swelling of the optic nerve with swelling and whitening of the adjacent retina and multiple foci of choroiditis (inflammation of the choroid). Her mantoux test was positive and her HRCT chest showed evidence of old tuberculosis infection. She was treated with anti-TB therapy for 9 months and her vision completely recovered, without any scarring or visual field loss. Therefore timely diagnosis and treatment can lead to excellent results.
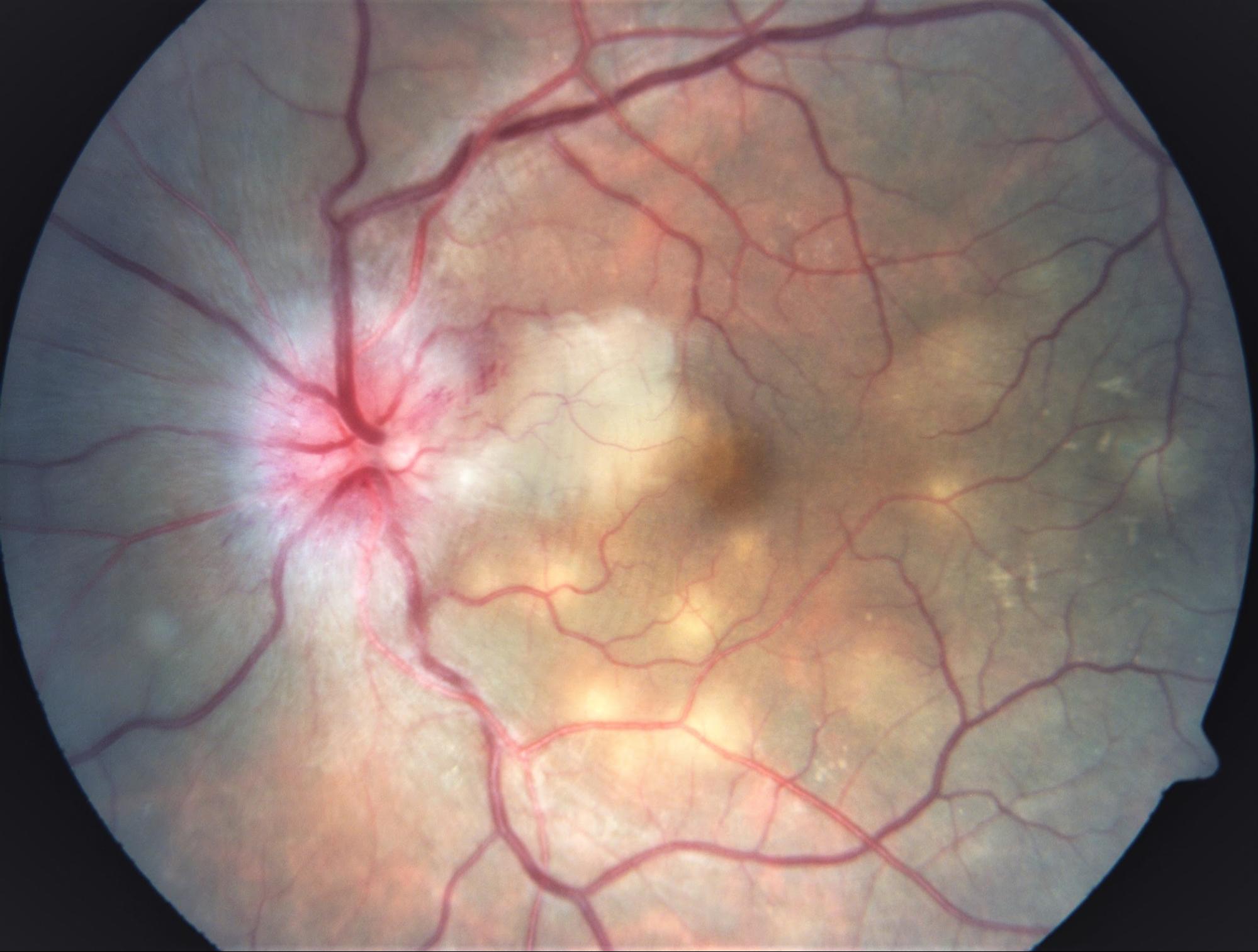
Neuroretinitis with choroiditis. Visual acuity : counting fingers at 2 metres
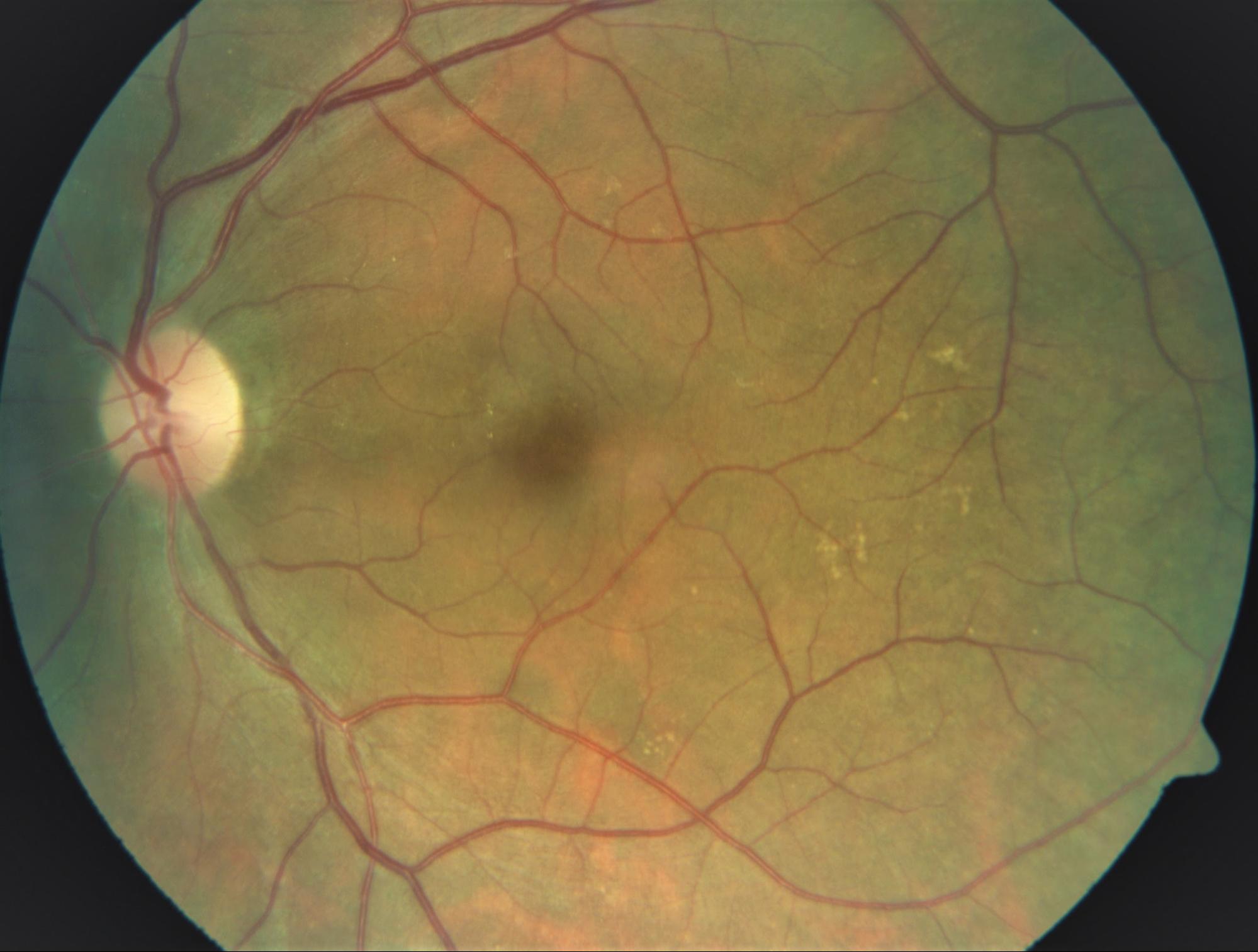
After 2 months of treatment. Visual acuity: 6/6
Case 2. A 47 year old gentleman presented with decreased vision in his right eye since more than 10 years but sudden loss of vision since 2 days. He had been treated several times for his eye problem with multiple courses of steroids at various hospitals in the past. On examination his right eye showed extensive scarring of the retina with a active edge of choroiditis passing through the macula (central, sensitive portion of the retina). His mantoux test was negative but HRCT chest showed evidence of tuberculosis. Hence he was treated with 9 month course of anti-TB therapy and his vision recovered completely, although with extensive scarring and visual field loss. In this patient because of delay in presentation, inappropriate treatment with steroids, there was extensive scarring of the retina, which could not be reversed even with treatment. However, patient recovered 100% visual acuity and further damage was prevented. It is therefore important to get the right treatment before complications of the disease develop.
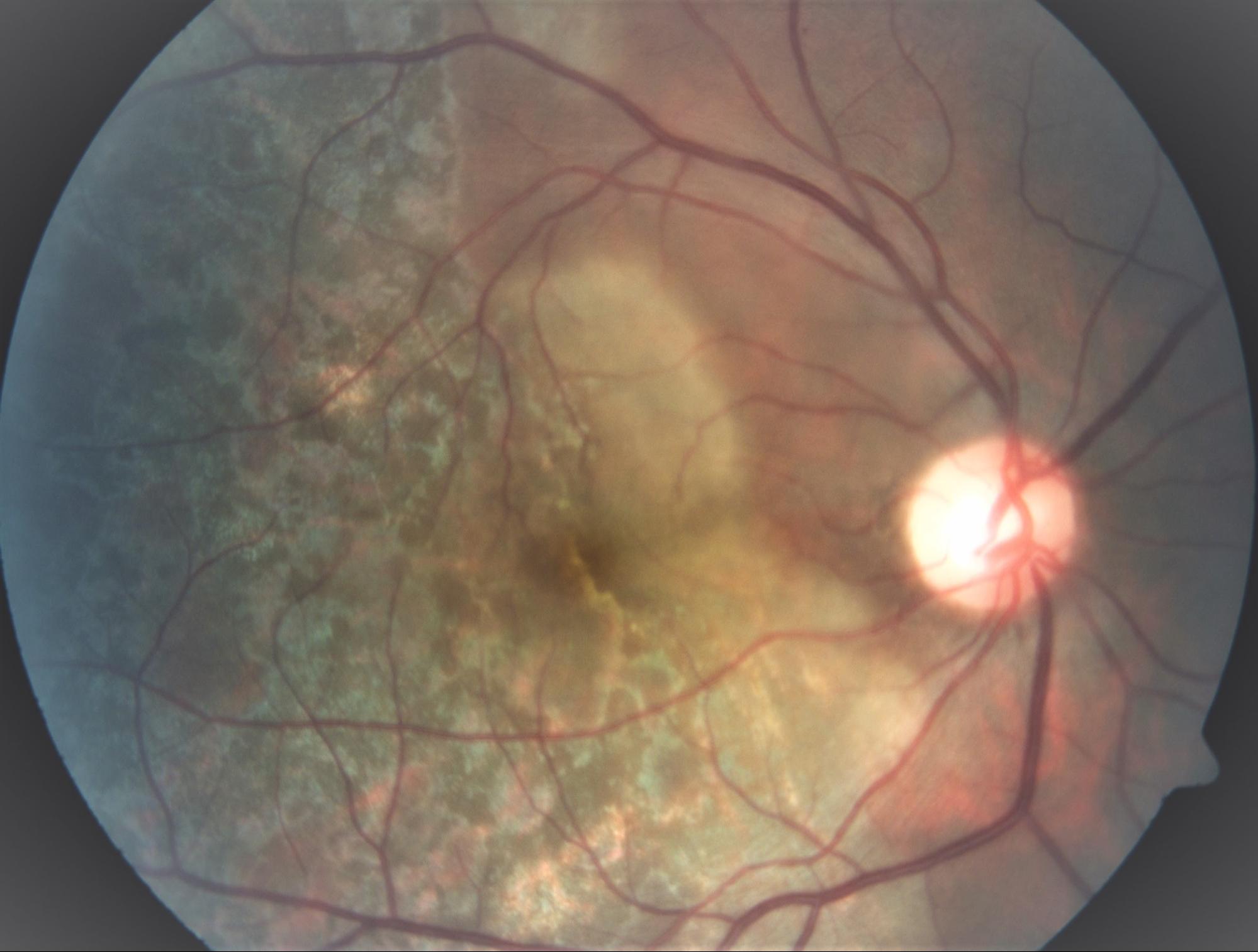
Extensive choroiditis with active edge. Visual acuity: hand movements
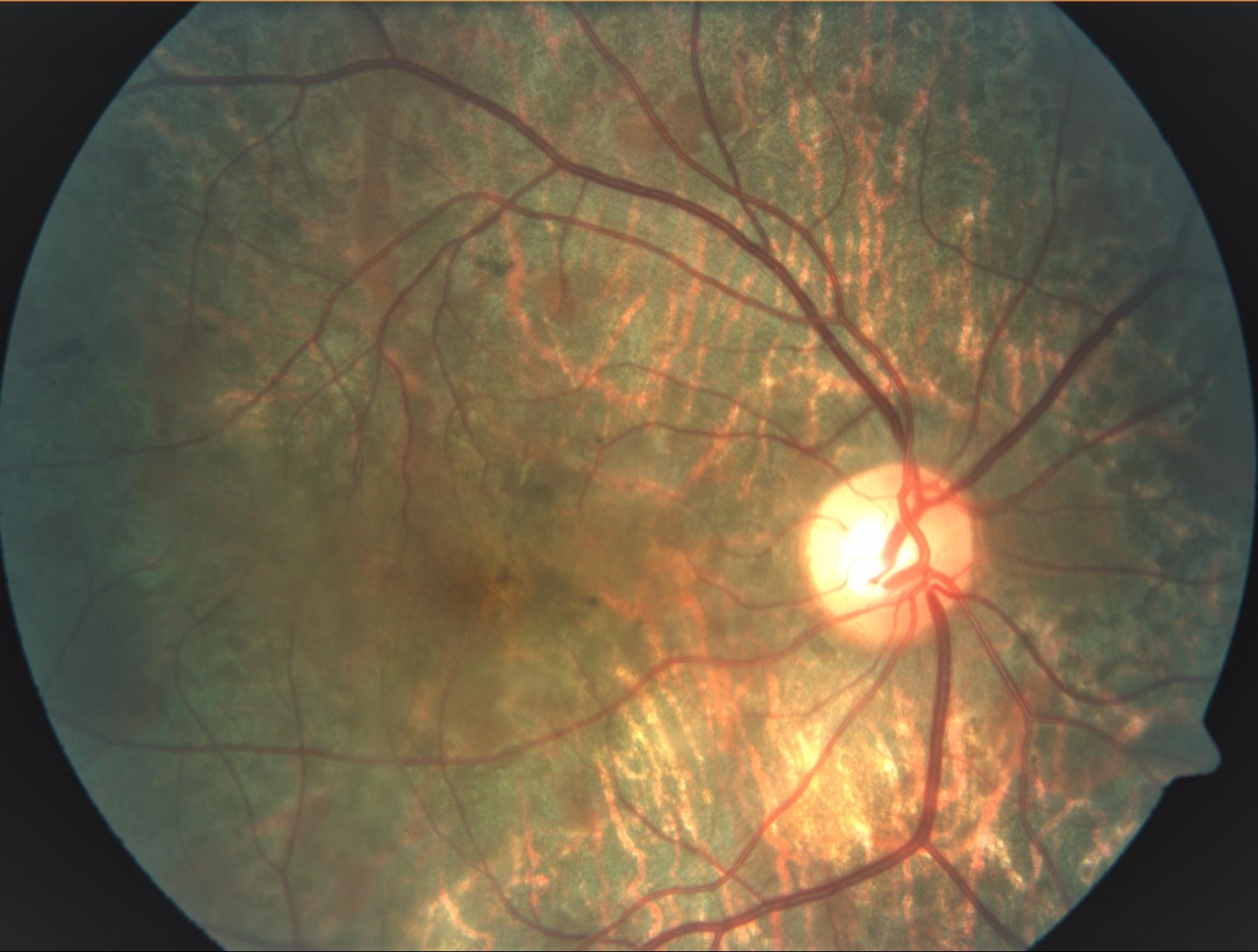
After 5 months of treatment. Extensive scarring, though visual acuity 6/6
Case 3. A 28 year old gentleman presented with severe redness, pain and reduced vision in his left eye since 15 days. He was being treated elsewhere with steroid eyedrops but to no avail. On examination his left eye showed inflammation of the sclera (white outer coat of the eye) with whitening in the adjacent cornea (transparent front portion of the eyeball, important for clear vision). He also had inflammation of the vitreous cavity (inner gel of the eye) and cystoid macular oedema (swelling of the centre of the retina). He complained of pain in the abdomen, radiating to the back since 1 year. His mantoux test was positive and guided by his abdominal symptoms we did an HRCT of the abdomen which showed multiple enlarged calcified lymph nodes and active TB with strictures in his kidney. We immediately started him on anti-TB treatment and referred him to the nephrologist. They agreed with our diagnosis and treated his kidney strictures with stent. He was relieved of his eye and abdominal symptoms in 3 weeks and his eye and kidney TB recovered fully with treatment. Timely diagnosis and treatment of TB is not only sight saving, it can also be life-saving.

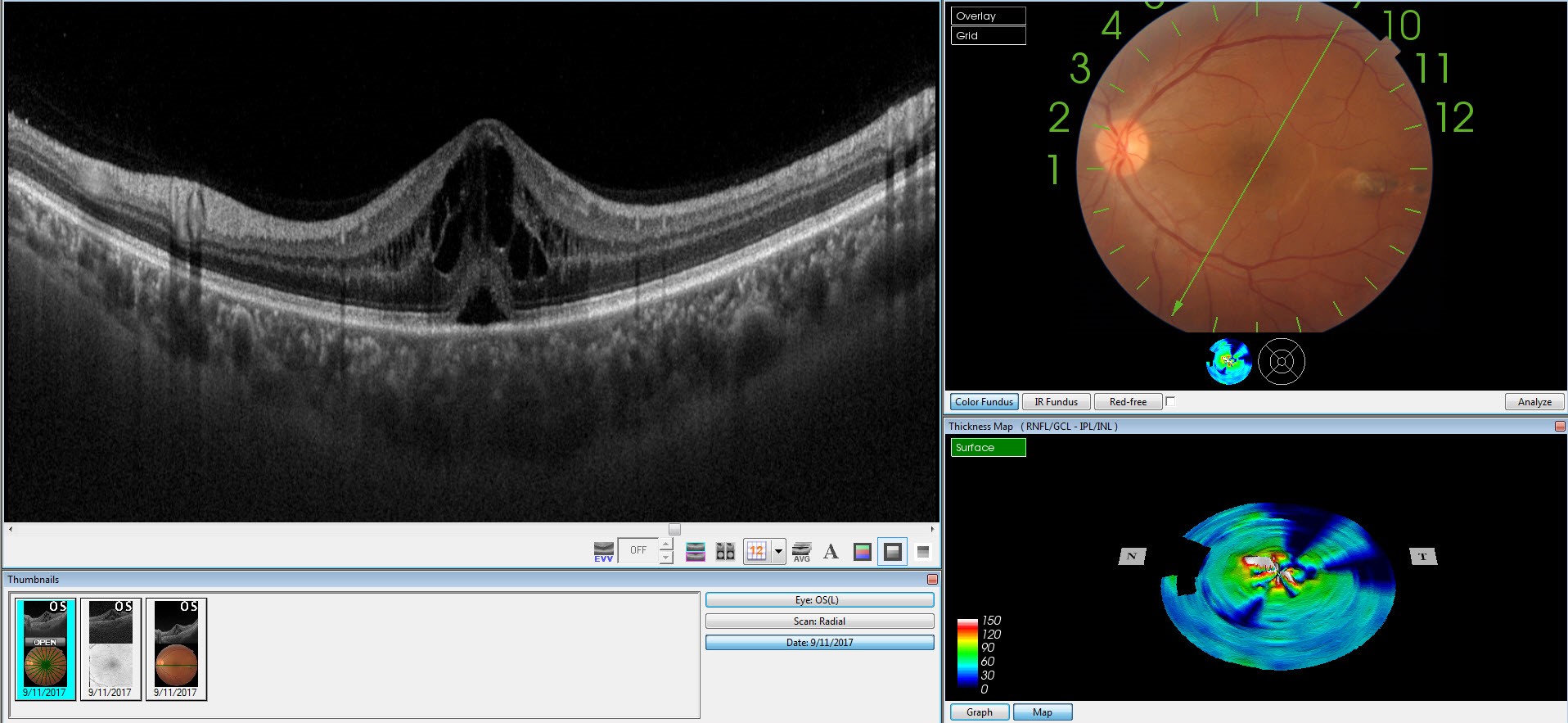
(Top) Sclerokeratitis (inflammation of the sclera and cornea) with (bottom) intermediate uveitis and cystoid macular oedema.

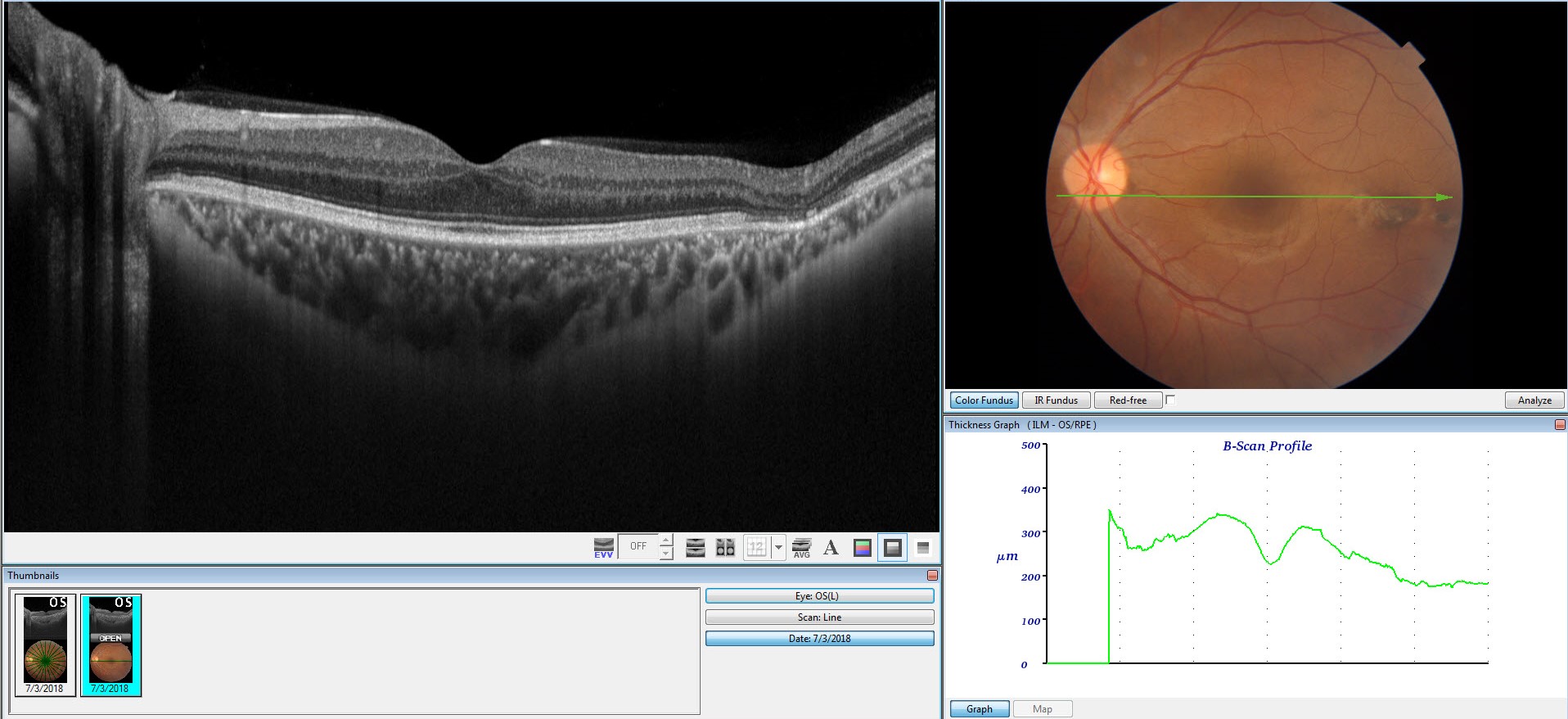
After 6 months of treatment. Completely resolved sclerokeratitis (Top) and cystoid macular oedema (bottom)
Ocular Tuberculosis cases highlight the fact that manifestations and clinical symptoms of the infection can differ drastically in patients. Hence, it needs a thorough examination, prompt diagnosis, and timely treatment. Early diagnosis and quick therapy can help in preventing further complications. Clinicians and ophthalmologists should be aware of such cases and findings when treating patients with this vision-threatening disease and patients with tuberculosis uveitis shouldn’t lose hope.
To continue reading on this subject, visit our next blog Ocular Tuberculosis Part 2
- A Simple Guide to Complicated Cataract Causesand Treatment - June 11, 2019
- Choosing the Right Intraocular Lens: Make an Informed Decision - February 28, 2019
- Intravitreal Injections: Indications, Procedure, Do’s, Don’ts and Myths - February 13, 2019



")
