Uveitis is the third leading cause of irreversible blindness. The incidence of blindness due to uveitis is 3% to 10% in developed countries and 25% in developing countries like ours. Despite the magnitude of the problem, few centers of excellence in diagnosing and treating patients with ocular inflammatory diseases exist. An exclusive Uvea Clinic was started at NEORETINA Eyecare Institute in July 2016, headed by Dr. Abhilasha, to bridge this gap for the patients. We believe:
What is Uveitis?

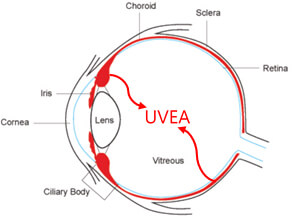
Uveal tract is the vascular middle coat of the eyeball. It consists of the iris (the part in the front of the eye that gives the eye its colour), ciliary body (behind the iris, responsible for making the fluid inside the eye) and the choroid (the vascular lining tissue encircling the retina). Inflammation of the inside of the eye, affecting one or more of these 3 parts of the uvea is called uveitis.
Prevalence of Uveitis
Uveitis, is the third leading cause of irreversible blindness worldwide. The incidence of uveitis varies from 14 to 52.4/100,000 with the overall prevalence around the world of 0.73%. Lack of awareness about uveitis and poor understanding of the disease and its management are the main reasons why a large number of cases remain undiagnosed/misdiagnosed and even progress to irreversible blindness.
Symptoms of Uveitis
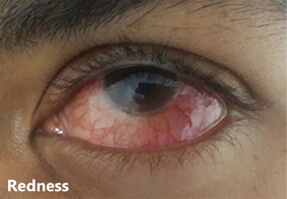
Symptoms of uveitis are very variable and may include any one or more of the following depending on the part of the eye affected: redness, decreased vision, pain, inability to see bright light and floaters.


Causes of Uveitis
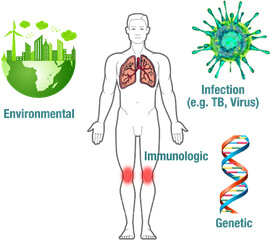
Uveitis occurs as a result of an immune reaction by our body to substances our body considers foreign. It can present following a huge spectrum of diseases. Genetic, infectious (tuberculosis, leptospirosis, viral and parasitic infections to name a few) environmental, systemic and immunologic diseases are some of the predisposing factors whose
association with uveitis has been proven.
Diagnosis of Uveitis
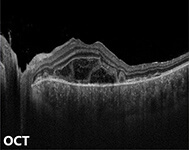
Finding the cause of uveitis in a particular patient is a tedious job involving eye scans such as fundus fluorescein angiography (FFA) and optical coherence tomography (OCT), blood tests, CT scans, and sometimes examination of a sample of fluid from the eye. Identifying the cause of uveitis is quite critical, since proper choice of treatment is so dependent on the underlying cause. Also because, treatment of one form of uveitis with a particular agent might be deleterious to the other. Hence patients need to cooperate with the treating specialist while he/she is able to identify the underlying problem.




Treatment of Uveitis
Infectious uveitis is treated with the appropriate anti-microbial tablets and steroid eyedrops, with or without steroid tablets. Uveitis (especially non-infectious or autoimmune) tends to be recurrent. In such cases, systemic immuno-suppressive therapy is combined with oral steroids to achieve long-term remission.

Medication should be taken only according to the doctor's advice and should never be started or stopped by the patient on his/her own.
Sometimes in cases of swelling in the retina due to uveitis, a steroid injection may be given to the outer coats of the eye (posterior subtenon triamcinolone). In more severe cases, steroid injection (intravitreal triamcinolone) or steroid implant (ozurdex) may be given to the inside of the eye.
In cases of retinal vasculitis, where blood supply to the retina is compromised, a retinal LASER may need to be done.
The treatment of uveitis may be prolonged and needs acceptance, persistence and cooperation from the patient as well as his/her family members.
Complications of Uveitis
As mentioned earlier, uveitis may lead to irreversible blindness. In fact, except cataract (opacification of the lens), all other complications of uveitis, including glaucoma (raised intraocular pressure leading to optic nerve damage) and macular oedema (swelling of the central part of the retina) may lead to irreversible loss of vision. Other complications
include vitreous opacification, formation of a membrane over the retina – ERM, macular scarring, loss of visual field and neovascularisation. Management of complications may require additional medical or surgical treatment.


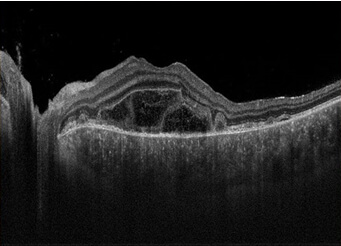
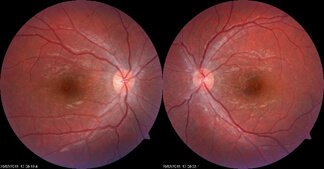
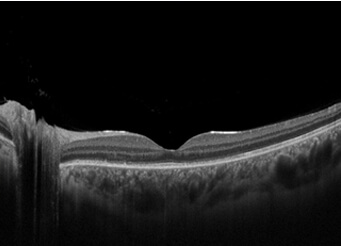
Clinical Examples treated at our centre
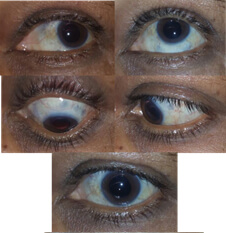
Condition: Fungal Nodular Scleritis
Before

After
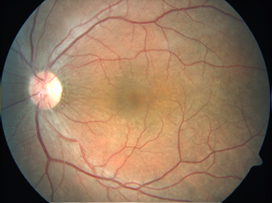
Leptospiral Panuveitis
Before

After
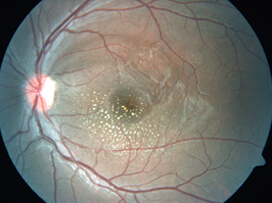
Rickettsial Retinitis
Before
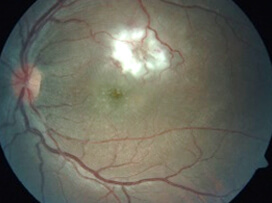
After
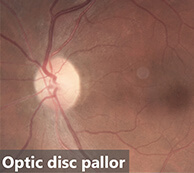
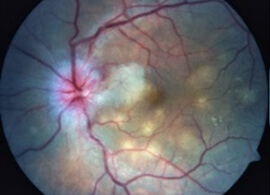
Tuberculous Optic Neuritis with Choroiditis
Before
After

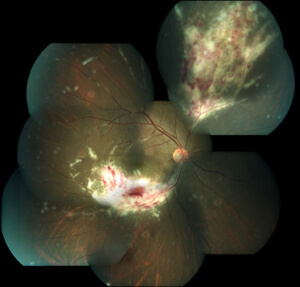
CMV Retinitis
Before
After
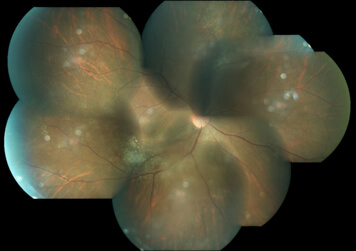
Vogt-Koyanagi-Harada Syndrome
Before

After
“I was highly impressed by the over all management of large number of patients properly guided and investigated very effectively. Staff at the reception and all management levels well trained and helpfully caring hardworking. My salute to all involved for starting proper management of large number of patients.”
SAROJINI UGALE
“The staff was very much kind and the clinic setup was very beautiful. Very nicely managed. I definitely would like to recommmed this clinic to my near and dear ones. Thanks once again for taking care of me!”
AZAM KHAN
“Excellent in all respects. Very clean and has well maintained toilets. The staff are very friendly and helpful. Overall extremely satisfying experience.”
SASIDHARA REDDY
“My dad had a retinal detachment which was found overnight and he had to undergo retinal detachment surgery (vitrectomy) within 7days. He flew down to Hyderabad and directly to Raja Ram Reddy. He suggested to go for surgery the very next day. It was a successful surgery and my dad got discharged in the evening. He is very cordial and really nice in speaking. He is calm cool minded. A perfect doctor to consult.”
NEHA PATNAIK
“I'm very happy with the drs approach and very patiently examined I have great confidence in Dr reddy its been three years that I come to Dr reddy all the way from Kolkata wish we have doctors like him at Kolkata too.”
ANIL KUMAR AGARWAL
“Best..Wonderful clinic with very helpful staff and well experienced and caring doctors like Dr.Srinivas and Dr.R.R.Reddy... I took my father who is diabetic and heart patient also for his eye surgery and the doctors guided us v.nicely to take care of him b4 & after surgery and my father's eyes r perfect...mashallah...thanks to God and then the neoretina team...Well done...keep spreading the light of vision in the life of others too. ”
MEHER ZAIDI
“I know her from since 3 years she diagnosed the retina detachment in my left eye and explained about the treatment. She works for NEORETINA eye care institute which is located in the nampally hyderabad. She clarifies each and every doubt of the patient patiently without any irritation. I mean some doctors gets irritated when the patient asks more questions but that's not the case with alka Rani madam. I suggest to all who are suffering from eye disorders to visit neoretina for timely treatment and speedy recovery.”
VASANTHI
“Excellent attention to my eye problem doctor Abhilasha Baharani at Neo Retina Eye Care Institute was very cooperative she is very echo friendly clear voice n determined i will in sha Allah refer to all of my near n dear to visit her if any one having eye problems i appreciate thanks a lot.”
MD MUZAFER
“Dr. Raja is one of the foremost experts in retina issues. He is very approachable at the same time gives you valuable advice.”
T PRASAD


